The size and number of polyps detected at VC are key to evaluating the risk of colorectal cancer. These factors distinguish patients needing referral to optical colonoscopy and polypectomy from those who can be sent home. As a result, polyp size measurement is closely related to VC's ability to detect clinically significant polyps as well as its cost-effectiveness as a screening method.
Virtual colonoscopy, unique in its ability to not only identify but also to measure polyps, permits risk stratification of patients according to polyp size, the most important predictive factor for malignancy in today's clinical environment, wrote Dr. Didier Bielen and his team from University Hospital Gasthuisberg, in Leuven, Belgium, along with colleagues from Siemens Healthcare (Journal of Computer Assisted Tomography, July/August 2008, Vol. 32:4, pp. 504-510).
"Patients with a lesion size of 10 mm or larger or with three or more lesions 6 to 9 mm in size have an elevated risk for cancer and should be referred for polypectomy," they wrote. "Patients with less than three lesions 6 to 9 mm in size can be offered either surveillance (i.e., control after three years) or polypectomy, depending on patient and/or physician preferences. All other patients are eligible for continued routine screening after five to 10 years."
However, manual measurement of detected polyps, usually done with the aid of electronic calipers, is time-consuming and variable between readers.
The study sought to evaluate the accuracy of an automated polyp size measurement tool and its effectiveness for risk stratification in 305 subjects (170 men and 135 women, mean age 57).
The subjects were recruited for an elevated familial risk of colorectal cancer (n = 57), surveillance after resection of colorectal cancer or polyps (n = 137), or symptoms suggestive of an elevated risk of the disease (n = 111).
All patients followed a low-fiber diet and one of three bowel preparation regimens. In the first group, 102 patients undergoing a classic bowel prep on the day of the exam were given 4 to 5 L of an electrolyte solution the day before scanning. A second group of 125 patients was given two doses of 45 mL of sodium phosphate as well as water-soluble iodinated contrast (3% meglumine ioxitalamate) for fecal tagging. A third group of 78 patients did not receive any laxatives but ingested 100 mL of the oral iodinated agent, meglumine ioxitalamate, the day before scanning.
Images were acquired on a 16-detector-row CT scanner (Sensation 16, Siemens Healthcare, Erlangen, Germany) using different scan protocols for dose reduction purposes. Scanning was performed at 120 kV, 55 mAs, and collimation of 0.75 to 1.5 mm. Alternately, images were acquired at 100 kV, 50 mAs, and collimation of 1.5 mm or 140 kV, 15 mAs, and collimation of 0.75 mm. Dose modulation (Siemens CARE dose) was used in 268 exams, CARE Dose 4D was used in 17, and 10 patients were scanned without dose reduction. Five patients were excluded for their large body habitus.
Polyp measurement
The measurement application functioned by first segmenting the polyp based on the difference in voxel densities at the interface between the polyp and the surrounding air, using a region-growing algorithm and "proprietary" enhancements.
"The next step was to fit the smallest possible bounding box containing the lesion using the maximum extension and the second maximum perpendicular to the first one to report maximum linear dimensions," they wrote. Then, the investigators applied three clicks to the polyp surface in the 3D endoluminal view for each kV and mAs setting used in the image acquisition, repeating the measurements for each window length and window level setting.
The measurement results were compared to the known sizes of the phantom polyps. In the patient group, the results were compared to independent measurements of the supine and prone datasets by two abdominal radiologists using two different window and level settings. Finally, the measurement results were applied to risk stratification, assigning polyps to a size group as described by the Workgroup on Virtual Colonoscopy. "Patients with lesions 10 mm or larger are referred for polypectomy, patients with lesions 6 to 9 mm might be eligible for short- or long-term follow-up," the group wrote.
|
|
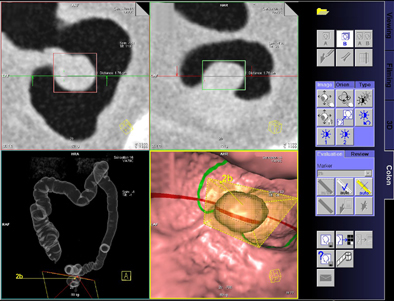
Graphic user interface shows automated measurement of a 17-mm polyp in coronal, axial, pseudo-double-contrast barium enema (DCBE), and endoluminal views. All images courtesy of Dr. Didier Bielen.
|
Equivalent accuracy
The results showed that the automated method produced accurate measurements compared to the manual method. In the phantom study, all measurements resulted in the same polyp size regardless of window or level setting. "Size deviation ranged from -11.43% to 14.29%, depending on kilovolt and milliampere second settings," Bielen and his team wrote.
For the study group consisting of 29 patients presenting with 40 polyps 6 mm or larger at colonoscopy, measurement of the polyps at colonoscopy ranged from 6.0 to 30.0 mm. The two radiologists overestimated some polyp sizes and underestimated others but achieved good correlation between the two measurement techniques (reader 1, y = 1.001x, with R2 = 0.72; reader 2, y = 0.929x, with R2 = 0.48), according to Bielen and colleagues.
The maximum automated measurements of the polyps ranged from 3.6 to 21.2 mm (mean, 9.5 mm), compared to manual measurements that ranged from 5.0 to 27.0 mm (mean, 9.7 mm) for reader 1 using the window width/level setting of 1700/-300 HU. Manual measurements ranged from 4.6 to 25.9 mm (mean, 9.3 mm) for reader 2 using the widow width/level setting of 1700/-300 HU and from 4.0 to 24.3 mm (mean, 8.2 mm) for reader 2 using the window width/level setting of 350/50 HU.
As for risk assessment, in the patient study reader 1 correctly classified 34 polyps in the appropriate size group versus 30 for reader 2, and 33 lesions in the automated measurements.
"The automated measurement tool provides an advantage over manual measuring because only one click on a lesion was necessary to measure it, avoiding time-consuming reconstruction, tilt, and spin of [multiplanar reformatted images] along the axes of the polyp," they wrote. "Although the automated size measurement categorized the patients to the correct size groups without any significant difference to the radiologist, it slightly improved patient risk stratification by reducing failed and unnecessary colonoscopy referral using the referral criteria as described by the Workgroup on Virtual Colonoscopy...."
Further study should be undertaken to determine "whether maximum linear dimension or polyp volume is the best indicator for cancer risk in polyps and the best parameter to determine if patients are eligible for future surveillance or routine screening," Bielen and his team wrote.
In the meantime, the lack of significant variation between human and automated results makes the automated method a useful and time-saving tool for polyp assessment, especially because little operator interaction is needed, they concluded.
By Eric Barnes
AuntMinnie.com staff writer
August 26, 2008
Related Reading
Automated polyp measurement cuts variability, May 21, 2008
Accuracy of polyp measurements depends on CT values, February 21, 2008
Colon polyps accurately measured using automated and manual 3D techniques, January 5, 2007
Polyp measurements more accurate in 3D, September 6, 2005
VC gets long-awaited reporting standards, November 2, 2004
Copyright © 2008 AuntMinnie.com
